

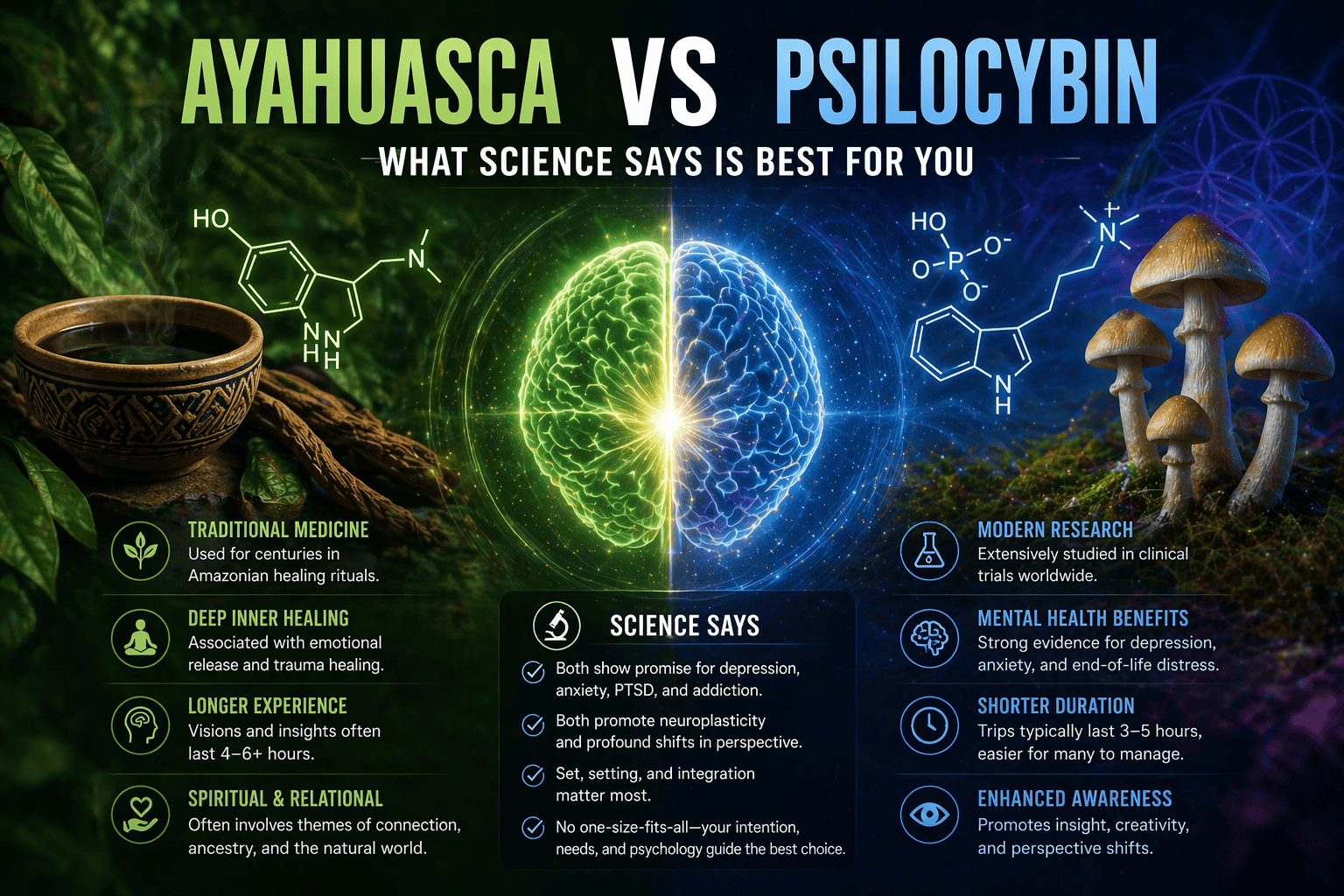
People often search ayahuasca vs psilocybin when weighing two powerful but very different paths. Both are classic psychedelics with long histories and modern research interest. The quick differences. Ayahuasca is a DMT brew activated by harmala MAOIs and usually taken in ceremony. Psilocybin comes from mushrooms and converts to psilocin in the body. Ayahuasca brings more purging and body load. Psilocybin tends to be gentler physically, easier to access, and better studied for depression and addiction in clinics [1][2][3][4].
Ayahuasca vs Psilocybin: Origins, Plant Sources, and Traditions
What Ayahuasca Is: Brew Components and Lineages
Ayahuasca is an Amazonian tea traditionally prepared by boiling the Banisteriopsis caapi vine with DMT-containing leaves such as Psychotria viridis or Diplopterys cabrerana. The vine contributes harmala alkaloids like harmine and tetrahydroharmine that act as reversible MAO-A inhibitors, which allow orally ingested DMT to become active [5][6]. The brew’s name can refer to the vine itself, the combined tea, or a broader healing tradition.
Lineages include Shipibo-Conibo, Quechua, Tukano and others across the Western Amazon. Ceremony is led by experienced healers who have trained for years. Songs known as icaros and the use of Amazonian tobacco are core elements, shaping attention and emotional flow throughout the night. Reports of visionary themes such as serpents, jungle motifs, and a powerful feminine presence are common in ethnographic and phenomenological accounts [7].
What Psilocybin Is: Mushroom Species and History
Psilocybin is a naturally occurring prodrug found in “magic mushrooms”. Once ingested, psilocybin is converted into psilocin, which engages serotonin receptors, especially 5‑HT2A, to alter perception and sense of self [8]. Species include Psilocybe cubensis, P. semilanceata, and P. mexicana. Uses are documented in Mesoamerican ritual life, with mid‑20th century accounts by Mazatec curandera María Sabina influencing Western awareness and research interest [9].
Over the past decade, psilocybin has moved back into clinical science with controlled studies for depression, end‑of‑life anxiety, and substance use, while mushroom retreats operate legally in a few countries today [1][2][3][10].
Traditional Uses vs Modern Therapeutic Contexts
Ayahuasca is still practiced within Indigenous and syncretic religious communities. In the United States, a handful of churches like União do Vegetal and Santo Daime have legal exemptions to serve the tea in their ceremonies following a 2006 Supreme Court decision, with additional federal and state rulings shaping access for specific congregations [11][12].
Psilocybin’s modern therapeutic context looks different. Oregon now licenses adult psilocybin services. Colorado is building a regulated natural medicine program. Multiple universities run clinical trials under FDA oversight for depression and addictions, while ketamine clinics offer a legal, related dissociative option now [2][3][13][14].
Ayahuasca vs Psilocybin Mushrooms: Pharmacology, Onset, and Duration
DMT, Harmala MAOIs, and Psilocin Explained
- DMT in ayahuasca. A short‑acting psychedelic when smoked, rendered orally active by harmala alkaloids that temporarily reduce gut and liver monoamine oxidase A. This creates a 4 to 6 hour visionary window with distinct somatic effects [5][6].
- Harmala alkaloids. Harmine, harmaline, and tetrahydroharmine extend and shape the state and can raise the risk for drug interactions due to MAO‑A inhibition [6].
- Psilocybin and psilocin. Psilocybin is dephosphorylated to psilocin, which binds to serotonin receptors, prominently 5‑HT2A. The result is altered sensory processing, emotional salience, and ego‑related networks that support insight and plasticity windows after dosing [8][15].
Onset, Peak, and Total Duration Compared
| Feature | Ayahuasca | Psilocybin mushrooms |
|---|---|---|
| Typical onset | 30 to 60 minutes | 30 to 90 minutes |
| Peak window | 1.5 to 3 hours | 2 to 3 hours |
| Total duration | 4 to 6 hours, sometimes longer | 4 to 6 hours, sometimes up to 8 hours |
| Notable body effects | Nausea, vomiting, diarrhea are common | Milder nausea, yawning, body warmth |
These ranges vary with brew strength, mushroom species and potency, personal metabolism, and whether meals were eaten shortly before dosing [5][8].
Tolerance, Microdosing, and Dose Ranges
- Tolerance. Classic psychedelics build rapid short‑term tolerance. Repeating full doses over consecutive days lowers effects. Cross‑tolerance occurs between psilocybin and other classic psychedelics [8][15].
- Microdosing. Sub‑perceptual or very low doses are popular, although controlled evidence remains mixed and often confounded by expectancy. Claims should be considered preliminary [16].
- Dose ranges. Psilocybin mushrooms vary. Common oral ranges for dried P. cubensis sit near 1 to 3.5 grams for moderate effects, with strong individual differences. Ayahuasca dose is usually measured by the cup during ceremony, yet potency swings widely by recipe and cook time. Start low, go slow is the wiser mantra here [5][8].
What the Experience Feels Like: Visuals, Emotions, and Purging
Ayahuasca often carries a palpable “medicine” feel. People describe heavy waves in the body, jungle‑like visuals, and a sense of being guided, sometimes by an unmistakably feminine intelligence. The purge can be loud. Buckets, retching, tears, and shaking are common. In Amazonian frames, this is cleansing rather than side effect [7].
Psilocybin tends to unfold as an inward canvas. Colors bloom. Sounds feel layered and close. Many report a soft dissolution of everyday boundaries and a reorganization of self‑stories. Physically, it is lighter for most, though waves of nausea or chill can arrive early and pass [1][8].
Set, Setting, and Intention Differences
- Set. Bring a clear why. Clarify intentions in a single sentence. Expect the unexpected. Ground and sleep well before dosing.
- Setting. Ayahuasca ceremonies emphasize darkness, music, and a communal container with defined roles. Psilocybin sessions in clinical or retreat contexts aim for low sensory input, eyeshades, and carefully curated music with trained support [1][2][17].
- Integration. Plan time to absorb. Journaling, therapy, nature, and community help translate insights into durable changes.
A guest once described an ayahuasca night this way. The room pulsed with singing, the lanterns were dim, and the rain on the roof felt like an extra instrument. Another person shared a mushroom session where a simple piano piece opened a flood of relief. Different paths, similar depth.
Ayahuasca and Psilocybin Comparison: Common Themes and Challenges
- Common themes. Mystical‑type experiences with unity and transcendence. Vivid autobiographical memory. Emotional catharsis. Fresh perspective on entrenched patterns [18].
- Challenges. Difficult somatics and purging with ayahuasca. Anxiety spikes or confronting grief with psilocybin. Both demand skillful support and preparation.
- Meaning making. The session is a catalyst. Outcomes depend on what happens before and after as much as during.
Ayahuasca vs Psilocybin for Depression, PTSD, and Addiction
Depression and Treatment-Resistant Cases
Psilocybin has the strongest clinical trial data so far. A phase 2 trial in treatment‑resistant depression showed significant symptom reductions compared with baseline after a single 25 mg psilocybin session plus psychotherapy, with effects visible at three weeks [3]. Another randomized trial comparing psilocybin to an SSRI found comparable or greater improvements on key measures in the psilocybin group at six weeks, though differences were not consistent across all endpoints [19].
Ayahuasca also shows promise. A randomized placebo‑controlled trial in Brazil reported rapid antidepressant effects within days among people with treatment‑resistant depression after a single dosing session [4]. Observational research suggests sustained mood improvements in naturalistic settings, though more rigorous trials are needed to establish durability and moderators of response [20].
Psilocybin vs Ayahuasca for PTSD and Anxiety
PTSD evidence for psilocybin is emerging and still preliminary, while MDMA is the primary psychedelic studied for PTSD. Psilocybin has stronger data for end‑of‑life anxiety and depression, where two randomized trials in patients with life‑threatening illness found large, sustained decreases in anxiety and depressed mood after a high‑dose session with therapy support [1][21].
Ayahuasca observational studies indicate reductions in anxiety and trauma‑related symptoms among ceremony participants, but randomized controlled trials are sparse. Existing reviews emphasize careful screening due to variable intensity and MAOI interactions [20][22].
Substance Use, Cravings, and Relapse Risk
- Psilocybin and alcohol use. A randomized clinical trial found psilocybin‑assisted therapy reduced heavy drinking days and increased abstinence compared with placebo plus therapy across 32 weeks [23].
- Psilocybin and tobacco. A small proof‑of‑concept study reported notable long‑term abstinence rates after psilocybin‑assisted therapy for smoking cessation, although larger trials are underway [24].
- Ayahuasca and addiction. Observational studies in ceremonial and therapeutic settings suggest reduced cravings and improved substance use outcomes, yet controlled trials are limited. Safety screening is essential given medication and cardiac considerations [22][25].
Safety, Side Effects, and Contraindications
Medication Interactions and Health Conditions
- MAOI interactions. Ayahuasca contains reversible MAO‑A inhibitors. Combining with serotonergic antidepressants can increase the risk of serotonin toxicity. Certain other drugs can also interact. Medical review and a taper plan are required before any ceremony [6][26].
- Lithium risk. Case reports suggest an elevated seizure risk when lithium is combined with classic psychedelics like psilocybin. Avoid this combination and seek psychiatric guidance for mood stabilizer management [27].
- Psychosis and mania. A history of psychotic disorders or bipolar mania is generally considered a contraindication. Family history warrants caution and professional consultation [26][28].
- Cardiovascular concerns. Both substances can raise heart rate and blood pressure. People with serious heart conditions need a physician’s clearance or should avoid use [26][28].
Nausea, Purging, and Physical Risks
- Ayahuasca. Nausea, vomiting, diarrhea, and tremors are common. The purge can be dehydrating and strenuous. Rare risks include arrhythmia or hypertensive events, especially with hidden drug interactions [6][22].
- Psilocybin. Transient nausea, headache the next day, and anxiety are most common. Severe medical events are rare in screened settings. The larger risks are unsafe environments and unaddressed mental health contraindications [1][26][28].
Screening, Preparation, and Integration Support
- Share a full medication list with a qualified clinician. Outcome. identify interactions and create a safe taper plan if appropriate.
- Clarify mental health history and goals during intake. Outcome. match to the right container and support team.
- Prepare mind and body. Outcome. reduce anxiety with orientation sessions, sleep, hydration, and a light pre‑dose meal plan.
- Decide on safety roles and boundaries. Outcome. agree on consent, touch policies, emergency plans, and privacy.
- Plan integration. Outcome. book therapy, peer support, or community circles within days after the session to translate insights.
The simple motto applies. Start low, go slow.

Legality, Access, and Cost in the United States
Federal Status, Decriminalization, and Exemptions
- Federal. Psilocybin and DMT remain Schedule I under federal law. Religious exemptions exist case‑by‑case for specific churches under the Religious Freedom Restoration Act and court rulings, including a 2006 Supreme Court decision involving UDV [11][12].
- State and city actions. Oregon launched licensed adult psilocybin services in 2023. Colorado passed a regulated natural medicine framework and began implementation, with services expanding through 2025. Decriminalization measures have passed in cities including Denver, Oakland, Santa Cruz, and Seattle, which affect enforcement priorities rather than create legal markets [13][14].
Clinical Trials, Ketamine Clinics, and Retreats
- Clinical trials. Psilocybin studies for depression and addiction continue at academic centers under FDA oversight. Participation can be free, but eligibility is strict [2][3][23].
- Ketamine. Legal off‑label use for depression and PTSD symptoms is available through clinics. While pharmacologically distinct, it offers a monitored psychedelic‑adjacent option [29].
- Retreats. Ayahuasca is offered legally in countries like Peru and Brazil within traditional and religious contexts. Psilocybin retreats operate in places like Jamaica and the Netherlands [20].
Ayahuasca Compared to Psilocybin: Availability and Cost
- Availability. Psilocybin services are now accessible to adults in Oregon, with Colorado expanding. Ayahuasca access in the United States is mostly limited to a small number of exempted religious groups or underground circles. International travel opens more options for both. Ayahusca is fully legal in Peru. Learn more: 10 Best Ayahuasca Retreats in Peru: Proven Safe Journeys
- Cost. As of 2025, Oregon psilocybin service sessions commonly range from about 1000 to 3500 dollars per high‑dose session including facilitation, while multi‑night ayahuasca retreats abroad often range from 1500 to 5000 dollars depending on location and support. These figures are editor‑verified and vary widely by provider. For a detailed breakdown of cost, check out: Ayahuasca Retreat Cost 2026: How Much Should You Pay?
Ayahuasca or Psilocybin: How to Choose Based on Your Goals
Therapeutic Goals, Support, and Risk Tolerance
- Goals. For structured depression or addiction treatment with evidence and defined protocols, psilocybin has more clinical backing today. For spiritual ceremony and Amazonian plant teachings, ayahuasca carries unique cultural depth [1][3][4].
- Risk tolerance. Ayahuasca demands more medical caution due to MAOI interactions and stronger body effects. Psilocybin has a milder physiological profile but still requires careful screening [6][26].
- Support. Choose teams with trauma‑informed skills and clear emergency plans. Licensed settings and vetted retreat staff reduce risk materially.
Ceremony, Retreat, or Clinical Model Options
- Ceremony. Traditional ayahuasca or mushroom circles emphasize ritual, music, and communal healing.
- Retreat. Hybrid models combine group preparation, multiple sessions, and integration days in a supportive environment.
- Clinical. Psilocybin services or trials use therapists, eyeshades, and curated music, with structured prep and follow‑up.
Psilocybin Compared to Ayahuasca: Accessibility and Integration
Psilocybin compared to ayahuasca is easier to access in regulated US settings and easier to integrate into psychotherapy, which makes it appealing for depression, anxiety near end‑of‑life, and substance use care. Ayahuasca offers a distinct ritual technology and worldview that some people seek precisely for its ceremonial intensity and community container [1][3][4][20].
Ayahuasca vs Psilocybin Retreat: Ceremony Formats and Facilitator Roles
Traditional Amazonian Ceremony Structure and Music
A typical night begins in silence with low light. The healer pours small cups, songs fill the room, and the arc of the night is shaped by icaros and careful attention. Helpers manage buckets and quiet voice guidance. The smell of mapacho tobacco is common. Safety means skilled oversight, boundaries, and clear consent practices [7][22].
Mushroom Retreats, Group Sessions, and Integration
Mushroom retreats range from ceremonial spaces to therapy‑informed programs. Common elements include group preparation, a dosing day with trained facilitators, and integration circles the next morning. Licensed service models in Oregon follow defined protocols for screening, preparation, facilitation, and post‑session processing. The tone is quieter, with eyeshades and music steering attention inward [13][17].
Beyond Ayahuasca vs Psilocybin: DMT, Ibogaine, Peyote, and Wachuma
Ayahuasca vs DMT vs Psilocybin: Overlap and Differences
- Smoked or vaporized DMT. Extremely rapid onset and a 5 to 15 minute peak, often described as a light‑speed launch into abstract or entity‑rich visions. The brevity demands experienced sitters and calm settings [30].
- Ayahuasca. Slower, relational, and embodied, with harmala alkaloids shaping the tone and length [6].
- Psilocybin. Middle of the road on duration with broad emotional and cognitive depth and fewer somatic challenges for most [8].
Ibogaine vs Ayahuasca vs Psilocybin: Intensity and Risks
Ibogaine is an indole alkaloid from Tabernanthe iboga used in structured detox contexts for opioid use disorder interruption. Effects can last 12 to 24 hours or longer, include strong ataxia and oneiric visions, and carry a known risk of cardiac arrhythmia through QT interval prolongation. Pre‑treatment cardiac screening and medical supervision are non‑negotiable [31]. Compared with ibogaine, ayahuasca and psilocybin present lower cardiotoxicity risks but still require screening and professional support [22][26].
Peyote and Wachuma vs Ayahuasca vs Psilocybin: Mescaline Paths
Peyote and San Pedro, known as wachuma in Andean traditions, contain mescaline and offer 8 to 12 hour experiences that are visual, empathic, and often heart‑centered. Peyote is at risk due to overharvesting and has deep significance for Native American Church communities. Non‑Indigenous people are encouraged to avoid peyote and consider cultivated San Pedro where legal, to reduce ecological and cultural harms [32].
Ethical Sourcing, Cultural Respect, and Sustainability
Indigenous Stewardship, Reciprocity, and Consent
- Respect lineages. Seek facilitators with direct training and consent from communities whose practices they carry. Ask how reciprocity and revenue sharing support Indigenous stewards.
- Consent and safety. Trauma‑informed practices, gender‑aware policies, and clear conduct codes protect participants and uphold tradition with integrity.
- Give back. Support Amazonian conservation and health initiatives that sustain the ecosystems and cultures that sustain the medicines.
Mushroom Cultivation, Foraging Ethics, and Safety
- Cultivation. Home cultivation where legal reduces pressure on wild populations and offers known species and potency.
- Foraging. Misidentification can be dangerous. Never consume wild mushrooms without expert identification. In the United States, contact a local mycological society or poison control if there is uncertainty [33].
FAQs: Ayahuasca vs Psilocybin and Common Questions
Is ayahuasca similar to psilocybin?
Both are classic serotonergic psychedelics with meaningful overlaps in mystical‑type experiences and therapeutic potential. Ayahuasca includes MAOI components and often produces strong purging and body sensations. Psilocybin is a single‑compound experience that tends to be gentler physically and more predictable in dose response [1][6][8].
Is ayahuasca the most powerful psychedelic?
Power is context dependent. Smoked DMT can be more intense moment‑to‑moment, while ibogaine can be more physically demanding and longer. Ayahuasca can feel especially profound due to ceremony, harmala effects, and duration. The right choice depends on intentions, health, and support [6][30][31].
Does psilocybin rewire the brain?
Rewire is a casual phrase. Research shows temporary increases in neural flexibility and connectivity, with decreases in rigid network patterns during the acute state, followed by windows that support behavior change when paired with integration. Some markers of neuroplasticity appear to rise in the days after dosing in animal and human studies [15][19].
Why shouldn’t you do ayahuasca?
Avoid ayahuasca if taking serotonergic antidepressants or other interacting drugs, if there is a history of psychosis or bipolar mania, or if there are significant cardiac conditions. Lack of trusted facilitators, unclear medical screening, or pressured settings are also reasons to postpone or choose a different path [6][22][26].
Conclusion: Key Takeaways and Safe Next Steps
Ayahuasca versus psilocybin is not a simple better or worse. Ayahuasca combines DMT with harmala MAOIs in a ceremonial container that many find spiritually catalytic, yet it carries more medical caveats and somatic intensity. Psilocybin mushrooms deliver a shorter, gentler physical profile, stronger clinical evidence for depression and addiction to date, and growing regulated access in the United States [1][3][4][23].
Recommendations Based on Different Use Cases
- Depression or alcohol use goals. Psilocybin with therapy in a licensed or research setting is the more accessible evidence‑based route for many.
- Spiritual ceremony with Amazonian roots. Ayahuasca with vetted, experienced facilitators and robust medical screening fits the intention.
- High medical complexity or interacting medications. Consider postponing, pursuing ketamine with medical oversight, or focusing on non‑drug modalities until conditions are optimized.
Here is the thing. Choose the container first, then the compound. The team, the screening, and the aftercare make the difference.
Resources for Education, Screening, and Support
- ClinicalTrials.gov for active psilocybin studies in the United States.
- Oregon Psilocybin Services program for licensed service center information in Oregon.
- Fireside Project for peer support during and after psychedelic experiences.
- SAMHSA National Helpline for mental health and substance use resources.
- Erowid and academic reviews by NIH and university centers for pharmacology and safety.
Methodology. This article synthesizes peer‑reviewed studies on pharmacology, clinical trials for depression and addictions, safety reviews on MAOI interactions and cardiac risks, and legal records related to religious exemptions and state programs. Claims about costs and availability are noted as of 2025 and editor‑verified where primary pricing data are limited.
Final takeaway. If ayahuasca vs psilocybin is still an open question, clarify your goals, get a medical review, vet facilitators, and plan integration before booking anything. Thoughtful preparation now pays dividends in outcomes later.
References
- Griffiths RR, Richards WA, McCann U, Jesse R. Psilocybin can occasion mystical‑type experiences having substantial and sustained personal meaning and spiritual significance. Psychopharmacology. 2006. doi:10.1007/s00213-006-0457-5
- Johnson MW, Griffiths RR. Potential Therapeutic Effects of Psilocybin. Neurotherapeutics. 2017. doi:10.1007/s13311-017-0542-y
- Goodwin GM, Aaronson ST, Alvarez O, et al. Single‑Dose Psilocybin for a Treatment‑Resistant Episode of Major Depression. N Engl J Med. 2022. doi:10.1056/NEJMoa2206443
- Palhano-Fontes F, Barreto D, Onias H, et al. Rapid antidepressant effects of the psychedelic ayahuasca in treatment‑resistant depression. Psychol Med. 2019. doi:10.1017/S0033291718001356
- McKenna DJ, Towers GHN, Abbott F. Monoamine oxidase inhibitors in South American hallucinogenic plants. J Ethnopharmacol. 1984. doi:10.1016/0378-8741(84)90003-0
- Riba J, Valle M, Urbano G, et al. Human pharmacology of ayahuasca. J Pharmacol Exp Ther. 2003. doi:10.1124/jpet.102.046431
- Shanon B. The Antipodes of the Mind, Charting the Phenomenology of the Ayahuasca Experience. Oxford University Press. 2002.
- Nichols DE. Psychedelics. Pharmacol Rev. 2016. doi:10.1124/pr.115.011478
- Carod‑Artal FJ. Hallucinogenic drugs in pre‑Columbian Mesoamerican cultures. Neurologia. 2015. doi:10.1016/j.nrl.2012.09.002
- Grob CS, Danforth AL, Chopra GS, et al. Pilot study of psilocybin treatment for anxiety in patients with advanced‑stage cancer. Arch Gen Psychiatry. 2011. doi:10.1001/archgenpsychiatry.2010.116
- Gonzales v. O Centro Espírita Beneficente União do Vegetal, 546 U.S. 418. 2006.
- Church of the Holy Light of the Queen v. Mukasey, No. 07‑35266, 9th Cir. 2009.
- Oregon Health Authority. Oregon Psilocybin Services. Program updates and rules. Accessed 2025.
- Colorado Natural Medicine Health Act. State implementation documents. Accessed 2025.
- Vollenweider FX, Kometer M. The neurobiology of psychedelic drugs. Nat Rev Neurosci. 2010. doi:10.1038/nrn2884
- Szigeti B, Kartner L, Blemings A, et al. Self‑blinding citizen science to explore psychedelic microdosing. eLife. 2021. doi:10.7554/eLife.62878
- Johnson MW, Richards WA, Griffiths RR. Human hallucinogen research. Psychopharmacology. 2008. doi:10.1007/s00213-007-0624-3
- MacLean KA, Leoutsakos J-MS, Johnson MW, Griffiths RR. Factor analysis of the Mystical Experience Questionnaire. J Sci Study Relig. 2012. doi:10.1111/j.1468-5906.2011.01653.x
- Carhart‑Harris RL, Giribaldi B, et al. Trial of Psilocybin versus Escitalopram for Depression. N Engl J Med. 2021. doi:10.1056/NEJMoa2032994
- Sarris J, Perkins D, Cribb L, et al. Ayahuasca and mental health. J Psychopharmacol. 2021. doi:10.1177/0269881120981385
- Griffiths RR, Johnson MW, Carducci MA, et al. Psilocybin produces substantial and sustained decreases in depression and anxiety in patients with life‑threatening cancer. J Psychopharmacol. 2016. doi:10.1177/0269881116675513
- Domínguez‑Clavé E, Soler J, Elices M, et al. Ayahuasca. A comprehensive review of pharmacological and neuroscientific literature. J Neurochem. 2016. doi:10.1111/jnc.13688
- Bogenschutz MP, Ross S, Bhatt S, et al. Psilocybin‑assisted treatment for alcohol use disorder. JAMA Psychiatry. 2022. doi:10.1001/jamapsychiatry.2022.2096
- Johnson MW, Garcia‑Romeu A, Griffiths RR. Long‑term follow‑up of psilocybin‑facilitated smoking cessation. Am J Drug Alcohol Abuse. 2017. doi:10.1080/00952990.2016.1170135
- Nunes AA, dos Santos RG, Osório FDL, et al. Effects of ayahuasca on addiction. J Psychoactive Drugs. 2016. doi:10.1080/02791072.2016.1180135
- Thomas KH, Leyton M. Pharmacological contraindications for psychedelic therapy. Pharmacopsychiatry. 2022. doi:10.1055/a-1897-9192
- Bonson KR, Murphy DL, et al. Seizures associated with lithium and psychedelics. Biol Psychiatry. 1996.
- Yaden DB, Griffiths RR. The subjective effects of psychedelics are necessary for their enduring therapeutic effects. J Psychopharmacol. 2021. doi:10.1177/02698811211018297
- Sanacora G, Frye MA, McDonald W, et al. A consensus statement on ketamine in mood disorders. JAMA Psychiatry. 2017. doi:10.1001/jamapsychiatry.2017.0080
- Strassman R. Human psychopharmacology of DMT. Biol Psychiatry. 1996. doi:10.1016/0006-3223(95)00409-3
- Alper KR, Lotsof HS, Kaplan CD. The ibogaine medical subculture. J Ethnopharmacol. 2008. doi:10.1016/j.jep.2008.02.009
- Terry M, Trout K. Cacti, conservation, and culture. Haseltonia. 2017.
- National Capital Poison Center. Mushroom poisoning overview. Accessed 2025.






 Your personalized retreat result
Your personalized retreat result